
MEN: Is Porn Addiction Real? What Research Actually Says About Problematic Porn Use in Men
Quick Answer
Porn addiction is not a DSM-5 diagnosis, but ICD-11 recognizes compulsive sexual behaviour disorder. If your use causes impairment, treat it as problematic and begin the 5-step plan today [1][2][3]. The goal is function first, not perfection.
Jump to: Compare definitions and tools | 5-step plan | FAQ
This is education, not medical advice.
Disclosure: MenTools publishes this article and may feature MenTools products.
How we evaluate: Products are assessed on nutrient form quality, dose vs NRV, authorised health claims, male-specific design, and independent research. Full sources are listed in the references below.
Quick Comparison
Key definitions, tools, and treatments at a glance.
| Item | What it is | Evidence level | Best for |
|---|---|---|---|
| ICD-11 CSBD | A recognized disorder code 6C72 with minimum 6 months of persistent, poorly controlled sexual behaviours causing marked impairment or distress [1] | International diagnostic consensus and expert review [2] | Men with clear functional impairment who need a clinical framework |
| DSM-5 stance | DSM-5 and DSM-5-TR do not include “porn addiction” or CSBD as a diagnosis [2][3] | Official manual position plus peer-reviewed commentary | Clarifying labels when discussing care in the U.S. |
| PPUS | Problematic Pornography Use Scale, a validated measure of impairment and dyscontrol linked to pornography use [4] | Peer-reviewed validation study | Self-assessment and tracking change |
| BPS | Brief Pornography Screen, a short screener to flag potential problematic use for further evaluation [5] | Peer-reviewed development and validation | Quick clinical or self-screening |
| Prevalence in men | Estimates vary by method and definition; robust population-level data remain limited, and ranges differ across studies [2] | Systematic reviews and position papers | Setting expectations and avoiding overgeneralization |
| Correlates and harms | Impairment can include relationship strain, reduced work or academic performance, and distress; perceived addiction is often influenced by moral incongruence [2][7] | Reviews and cross-sectional studies | Distinguishing distress from functional impact |
| CBT and ACT | Structured therapies that target thoughts, urges, values, and skills; evidence supports benefit for CSBD and related behavioural dyscontrol [2] | Clinical reviews and emerging trials | Skills-focused change and relapse prevention |
| Peer support | Groups provide accountability and shared strategies; benefits vary by fit and engagement | Observational and practice-based evidence | Ongoing support and accountability |
| Blockers and habit tools | Filters, timers, and friction can reduce cue exposure and make habits harder to trigger | Behaviour change literature on habit formation averages 66 days to stabilize [6] | Fast-start environmental changes |
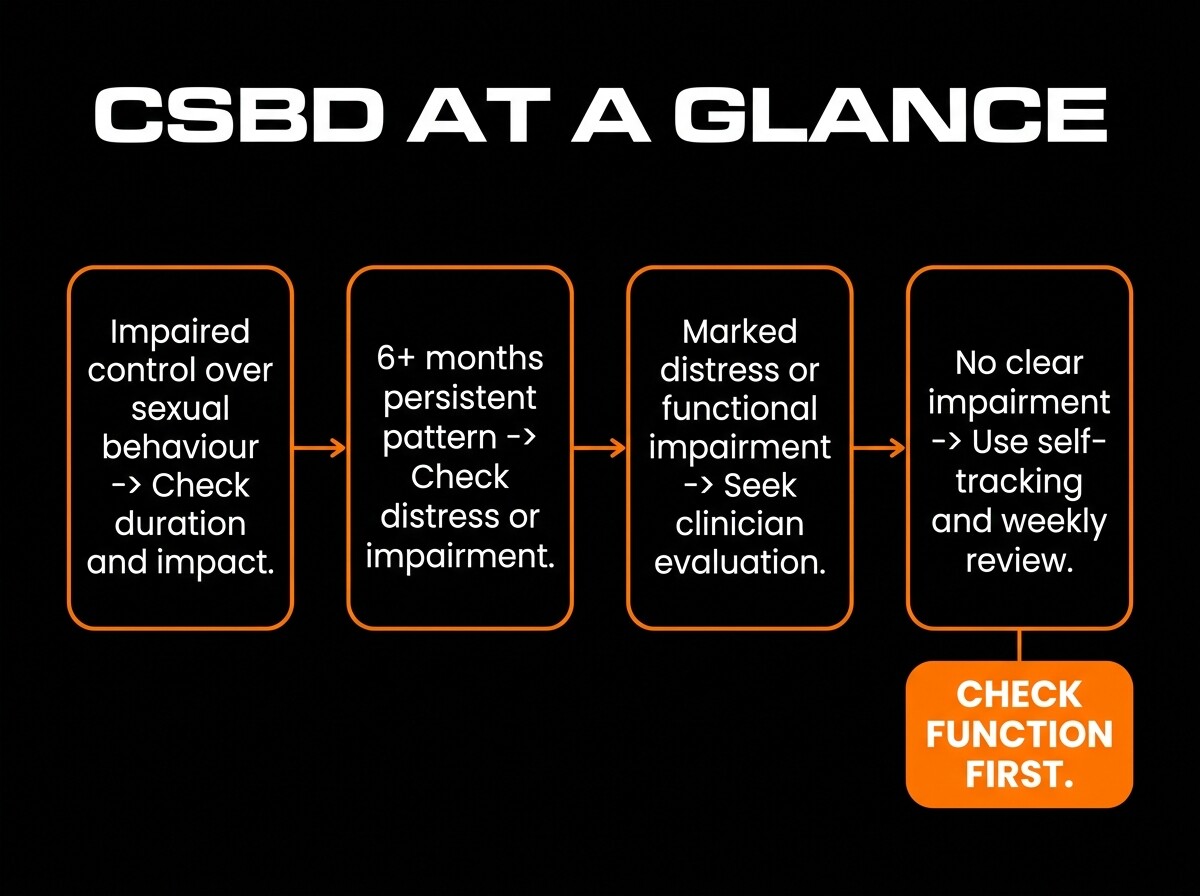
CSBD at a glance: ICD-11 criteria, 6-month threshold, and decision triggers to seek evaluation.
The Real Answer
Is porn addiction recognized by DSM or ICD?
DSM-5 and DSM-5-TR do not list porn addiction or CSBD, so clinicians in DSM-based systems may use related codes or describe symptoms without a formal diagnosis [2][3]. ICD-11, effective internationally since 2022, includes CSBD under code 6C72 [1].
What is CSBD and how is it diagnosed?
ICD-11 defines CSBD as a persistent pattern of failing to control intense sexual impulses or behaviours resulting in marked distress or impairment, with a minimum duration of 6 months [1]. It does not hinge on a specific behavior like porn alone, but pornography can be part of the pattern [2].
How common is problematic porn use in men?
Prevalence estimates vary widely because measures and thresholds differ, and many studies rely on self-perception rather than impairment [2]. Reviews stress caution, noting that population-level rates depend on criteria that distinguish distress from functional impact [2].
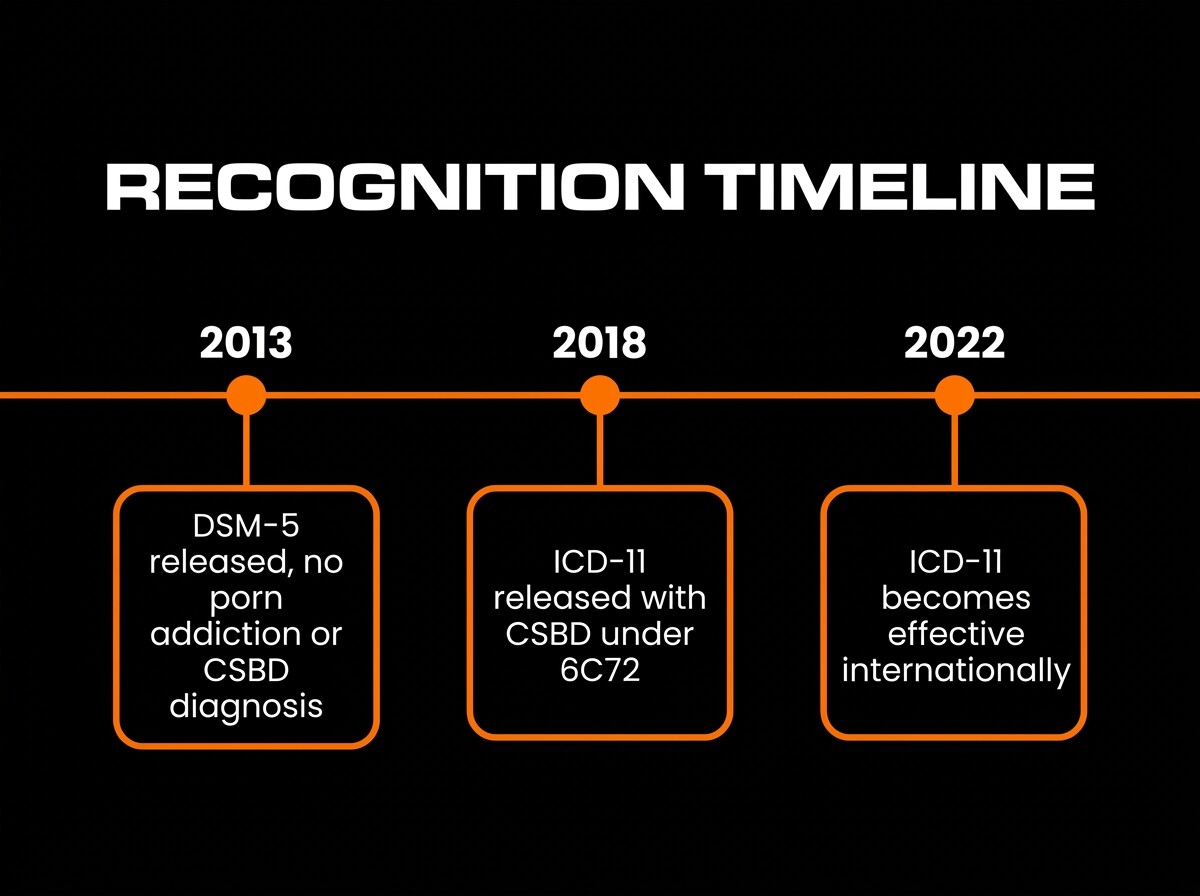
Recognition timeline: DSM-5 (2013), ICD-11 release (2018), ICD-11 effective (2022) with CSBD recognition.
What predicts distress versus impairment?
Perceived “addiction” to porn often tracks moral incongruence rather than use frequency alone, which can inflate distress without corresponding functional impairment [7]. Function-based criteria like missed work, relationship impacts, or inability to meet obligations better mark problematic use [2].
Which treatments show benefit in studies?
CBT and ACT appear helpful for CSBD by targeting habits, triggers, values, and coping skills, with evidence emerging from clinical reviews and early trials [2]. Medication may be considered for co-occurring conditions, but speak with a qualified clinician for individualized care [2].
Why This Fails
All-or-nothing rules create rebound use, shame loops, and secrecy. Unaddressed anxiety, sleep loss, and easy access keep urges cued and strong.
Without values-based alternatives, turning off porn leaves a vacuum that stress fills. Real change sticks when triggers are reduced and replacements matter.
How to Fix It
The Simple Framework
Reduce triggers, build alternatives, and add accountability. Aim for functional wins each week, not perfection.
Put time and friction between cues and urges, and make valued actions easier than default habits. Review progress every 7 days.
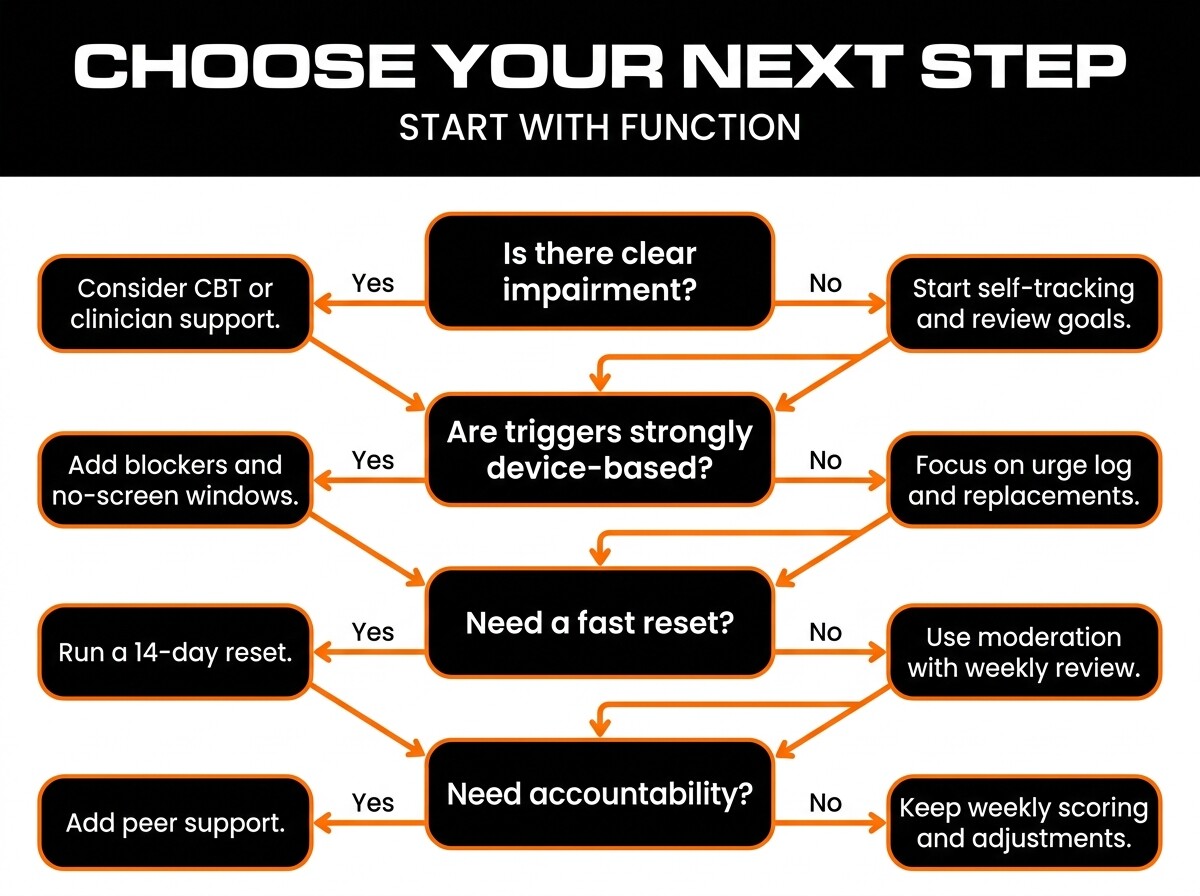
Decision flowchart: choose your next step based on impairment, distress, and goals.
5-step plan
- Define impairment and goals. Write specific impacts on work, relationships, mood, and set 1 to 2 measurable weekly targets.
- Track urges and contexts. Log time, device, location, emotion, and outcome for 14 days to reveal patterns.
- Modify cues and devices. Add site blockers, remove private-browsing defaults, and schedule no-screen windows.
- Replace with valued actions. Plug in short, rewarding alternatives like exercise, learning, or social time that align with your values.
- Review weekly and seek care if needed. Score impairment and progress, then adjust; if impairment persists, consider CBT or a clinician consult.
Who this is for:
- Men experiencing impairment in work, school, or relationships
- Men who want practical, values-driven tools
- Men open to tracking and accountability
- Men unsure whether to quit or moderate
Who this is not for:
- Anyone at immediate risk of harm or coercive sexual behavior
- Those with severe depression, suicidality, or crisis without professional support
- Men seeking medical instructions or medication changes
- Individuals looking for guaranteed cures
FAQ
Can you be addicted to porn?
Porn addiction is not a DSM-5 diagnosis, but CSBD in ICD-11 recognizes a pattern of impaired control over sexual behavior that may include porn [1][2]. Focus on impairment and duration, not labels.
Is quitting required or can moderation work?
Both approaches can work. Choose the smallest effective change that reduces impairment and supports your values, then adjust with weekly reviews [2].
Does porn cause erectile issues?
Evidence is mixed. Some papers suggest associations between heavy online porn use and sexual dysfunction, while others find limited or no direct causal links [9][10].
How do filters and blockers help?
They add friction and reduce cue exposure, which supports habit change. Behaviour research suggests habits often need sustained repetition over weeks to stabilize, averaging 66 days in one study [6].
What about partners and disclosure?
Share impacts and goals, not confessions alone. Use specific boundaries and accountability, and consider couples support if your partner is affected [2].
When should I see a clinician?
Seek care when impairment persists over months, when urges feel unmanageable, or when co-occurring issues like anxiety or depression are present. Speak with a qualified clinician for assessment and options [2].
Is faith-based recovery compatible with therapy?
Yes. Values can guide goals, while therapy adds skills and structure; avoid shame-based rules that backfire and focus on function [2][7].
Final Recommendation
If porn use is impairing your life, follow the 5-step plan and consider CBT with a clinician experienced in CSBD. Track function weekly and adjust until you see consistent gains [2].
Options For Men to Take Action
- Fast start: install a blocker, set device friction, and do a 14-day reset with a daily urge log.
- All-in-one: structured CBT plus accountability for values, triggers, and relapse prevention skills with the MenTools Quit Porn Protocol
- Low-cost: self-tracking with the MenTools Quit Porn Protocol, peer support and weekly reviews to hit small, repeatable wins.
If you want to go deeper on porn recovery and habit change, explore the MenTools Habits hub for guides and frameworks built specifically for men.
To support your daily routine with targeted nutrition, explore MenTools One A Day, formulated with chelated minerals and active B-vitamin forms for men.
When you are ready to turn ideas into action, start a focused challenge or daily routine inside the MenTools app and track how consistent habits change how you feel.
Last updated: 2026-03-03 v1.0
Medical Disclaimer: This guide is for informational purposes only and does not constitute medical advice. Always speak with your doctor or another qualified healthcare professional before starting any new supplement or programme if you have medical conditions or take prescription medication.
References
- [1] World Health Organization. ICD-11, 6C72 Compulsive sexual behaviour disorder. https://icd.who.int/browse11/l-m/en#/http://id.who.int/icd/entity/1630268048
- [2] Kraus, R., Krueger, R., et al. Compulsive sexual behaviour disorder in ICD-11. World Psychiatry. 2018. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6120155/
- [3] American Psychiatric Association. DSM-5-TR resources. https://www.psychiatry.org/psychiatrists/practice/dsm
- [4] Kor, A., Zilcha-Mano, S., et al. Problematic Pornography Use Scale: Psychometric examination. Addictive Behaviors. 2014. https://pubmed.ncbi.nlm.nih.gov/24799194/
- [5] Kraus, R., Martino, S., Potenza, M. Development and validation of the Brief Pornography Screener. Addictive Behaviors. 2017. https://pubmed.ncbi.nlm.nih.gov/28531871/
- [6] Lally, P., van Jaarsveld, C., Potts, H., Wardle, J. How are habits formed in the real world? European Journal of Social Psychology. 2010. https://onlinelibrary.wiley.com/doi/abs/10.1002/ejsp.674
- [7] Grubbs, J., Exline, J., Pargament, K. Moral incongruence and perceived addiction to pornography. Psychology of Addictive Behaviors. 2015. https://pubmed.ncbi.nlm.nih.gov/25705986/
- [9] Park, B. Y., Wilson, G. The impact of internet pornography on sexual function: A review. Behavioral Sciences. 2016. https://pubmed.ncbi.nlm.nih.gov/27527226/
- [10] Landripet, I., Stulhofer, A. Pornography use and erectile dysfunction among young men. Journal of Sexual Medicine. 2015. https://pubmed.ncbi.nlm.nih.gov/25652606/

